A dental consent form comes home in a backpack.
Maybe it is folded between a lunch menu and a field trip notice. Maybe a parent sees it after work while making dinner, checking homework, and sorting through a stack of school papers. The form says dental care is available at school, but questions come quickly:
Is this really free?
Who will see my child?
What if my child is scared?
Is this just a screening?
What happens if they find a cavity I cannot afford to fix?
For those of us working in children’s oral health, it is easy to see a missing consent form as a missed opportunity. But our Dental Resource Program members know the story is usually more complicated.
A recent JAMA Network Open study of more than 63,000 Medicaid-enrolled children in the Bronx highlighted a troubling paradox in school-based oral health care: children without prior dental visits were less likely to participate in school-based caries prevention programs, even though they may be among the children most likely to benefit.
That finding raises an important question: if school-based dental programs are designed to reach children who face barriers to care, why are some of those children still missing out?
To help answer that question, we turned to the experts who see these barriers every day — nonprofit dental clinics and community-based providers in our Dental Resource Program. The organizations that responded serve tens of thousands of children each year through school-based dental care in marginalized communities across the country.
Their insights remind us of something important: when consent forms do not come back, the reason is rarely as simple as “parents don’t care.”
More often, the form never made it home. Or the parent was overwhelmed. Or the family did not understand what was being offered. Or they feared a bill would arrive later. Or they worried that a school visit would identify a problem they still could not afford, schedule, or access.
The consent problem often starts before a parent has the chance to say yes or no.
A paper form placed in a backpack may not make it home. If it does, it lands alongside homework folders, lunch menus, sports forms, behavior updates, and other school communications. For a parent working long hours, caring for multiple children, or managing an unstable home life, one more form can easily disappear.
At Ready Set Smile in Minneapolis, Minnesota, Tessa Trepp Wetjen sees that reality often.
“Families have so much coming at them,” Trepp Wetjen said. “A consent form can get buried in all the paperwork coming home from school. Some parents may also assume the program isn’t meant for them or that their child doesn’t need it.”
Dr. Wanda Cloet, DHSc, RDH, of Central Community College in Hastings, Nebraska, pointed to a similarly simple but common barrier: parents may not check their children’s book bags. Teresa Bell of Gateway to Oral Health Foundation in St. Louis, Missouri, also noted that when students are responsible for transporting forms, there is always a chance the paperwork will be lost or simply never returned.
For some families, the communication chain is even more fragile. Amie-Jo Leshovsky of Apple Tree Dental in Minnesota said guardianship changes can interfere with care when a child’s responsible party changes, but the dental office does not receive updated information.
These are not signs of indifference. They are signs that a one-time paper form is often too fragile a system for reaching families whose lives may include shifting contact information, multiple caregivers, transportation challenges, or other competing demands.
One of the most important things our members emphasized is that low consent return should not be confused with lack of concern.
Even within dentistry, it is not uncommon to hear assumptions that parents whose children have untreated dental disease must be lazy, irresponsible, or unconcerned. But the providers working closest to these families describe a different picture.
Holly Jorgensen, CRDH, Executive Director of Let’s Smile, Inc. in Owatonna, Minnesota, said the most common barriers are usually about access, communication, and life circumstances.
“The children who need care the most are often in families experiencing the highest levels of instability,” Jorgensen said. “That instability directly affects whether a form gets home, whether contact information is current, and whether a parent has the time and clarity to respond.”
That perspective matters. Many parents want what is best for their children, but they are juggling rent, food, work schedules, school messages, medical appointments, transportation, language barriers, and the daily pressure of getting everyone through the week.
A dental consent form may be important, but it is competing with everything else that keeps a family afloat.
That does not mean the need for dental care is any less urgent. It means the consent process must be designed for real families, not ideal circumstances.
Our members also reminded us that dental professionals sometimes forget how complicated dental care can seem to people outside the field.
Parents may not understand the difference between a school dental screening and enrollment in a comprehensive school-based dental program. They may not know whether a visit includes prevention, diagnosis, restorative care, or only a visual screening. They may not understand why primary teeth need treatment if they will eventually fall out.
Dr. Cloet offered one telling example. She heard from a parent who assumed that because their child sees an orthodontist, preventive services such as fluoride varnish or sealants were already being addressed.
“To those of us in dentistry, it sounds almost funny because we know orthodontic care and preventive care are completely different,” Cloet said. “But for parents, it can all fall under the same broad category of ‘dental.’ That tells us we need to do a better job explaining what services are being offered and why they matter.”
That kind of confusion is not irrational. It reflects how complicated dental care can feel from the outside.
Amanda Holding, Director of Dental Services and Healthy Futures at Heartland Community Health Center in Lawrence, Kansas, sees a related challenge. Families may confuse an annual school dental screening with enrollment in a more comprehensive school-based dental program.
“We have to be very clear about the difference between a screening and comprehensive care,” Holding said. “Parents need simple, direct information about what the program does and what their child will receive.”
Other misconceptions involve the care setting itself. Bell said some parents ask whether actual dentists provide care through mobile programs, while others doubt whether restorative services can be performed in dental vans. For parents familiar only with a traditional dental office, a school-based or mobile model may require extra explanation.
That is especially true when children are not in pain. Leshovsky said some parents do not understand why primary teeth need treatment if they will eventually fall out. She also hears misconceptions about fluoride and silver diamine fluoride.
“Education is a big part of this,” Leshovsky said. “Parents need to understand why primary teeth matter and why preventive services are important before a child is in pain.”
That is a powerful reminder for anyone working in children’s oral health: consent materials should not merely request permission. They should help parents understand why care matters, what services will be provided, and what happens if additional treatment is needed.
Even when services are free or covered, families may be cautious. Many have had experiences with confusing healthcare bills, insurance limitations, or unexpected charges. For those families, signing a healthcare-related form may feel risky.
Trepp Wetjen said one of the biggest concerns she hears is fear that the service will cost something or that a bill will arrive later.
“That fear is real,” she said. “Families want to know they are not signing up for a surprise bill.”
Kathryn Dolan of Tufts University in Boston also identified financial uncertainty as a major barrier, especially for families without dental insurance or those unsure about what Medicaid will cover. Leshovsky added that knowing whether services are covered 100% can make a major difference in whether parents feel comfortable saying yes.
This is why programs may need to be more explicit than they think. A single phrase such as “free dental care” may not be enough. Families may need repeated reassurance that they will not receive a surprise bill.
Cost is not the only concern. Consent is also an act of trust.
For many parents, especially those who have had negative experiences with healthcare systems, school systems, or government-related paperwork, signing a form may raise concerns that go beyond dentistry. Dolan said undocumented families may be hesitant to sign forms because of fears about documentation or exposure. Others may have a broader distrust of healthcare systems or school-based programs.
Several providers said families sometimes want to be there during the child’s appointment. Others want reassurance that treatment will not be forced if a child is afraid, uncomfortable, or resistant.
“Parents want to know their child will be safe and respected,” Dolan said. “For some, the concern is not whether dental care matters. It is whether they understand what will happen and whether their child will still have a voice.”
Those concerns deserve respect.
Programs can help by clearly explaining what happens during the visit, who provides care, how children are comforted, what services may be performed, and how parents will be contacted if additional needs are found.
But trust is not built by one form alone. It is built through relationships — with school nurses, community health workers, bilingual staff, familiar providers, and clinics that families can return to over time.
For families facing significant barriers, agreeing to a school-based dental visit may raise another concern: what happens if the program finds a cavity or identifies a treatment need?
A screening without an accessible care pathway can feel like one more problem to solve. Parents may already suspect their child needs care. But if they do not know where to go, how to pay, how to get time off work, or how to arrange transportation, confirmation of the problem may feel overwhelming rather than helpful.
Trepp Wetjen put it plainly: families need to understand whether participation helps their child or simply reinforces what they already know.
“Families want to know if saying yes will actually help,” she said. “Are we providing a service, or are we just confirming a need they already have trouble getting addressed?”
That is why the connection to a dental home is so important.
At America’s ToothFairy, we believe children need more than one-time care events. A dental home provides an ongoing relationship and continuity of care with a dental provider or clinic where children can receive preventive care, treatment, follow-up, and support over time.
Leshovsky emphasized that continuity from a rural perspective.
“Staying with the same provider is necessary,” she said. “Compliance is very difficult if a program comes in and only completes preventive services and the family then has to find a different provider to complete the treatment.”
A dental home is not just a place for follow-up. It is part of the relationship that helps families trust that saying yes will lead to care, not another burden.
The JAMA study and the field experience of our Dental Resource Program members point to the same concern: the children most likely to benefit from school-based care may still be missed when participation depends on systems that do not reflect family realities.
That should challenge all of us who care about access to dental care for children.
The answer is not to blame parents. The answer is to build consent systems that are easier to understand, easier to complete, and more responsive to the realities families face before a child ever sits in the dental chair.
Our members are already showing what that can look like in practice. Some use text messages with direct enrollment links, QR codes on postcards, easy online forms that do not require a login, and paper forms for families who prefer them. Others attend school events so parents can ask questions in person, distribute consent forms during enrollment or at the beginning of the school year, or use universal forms that allow families to respond “yes” or “no” so every parent has a real opportunity to be heard.
Many also work through trusted messengers. As Dr. Wanda Cloet put it, “School nurses are the key.” School nurses, social workers, office staff, Head Start teams, Community Health Workers, and bilingual staff can help families understand what is being offered, why it matters, and how to complete the process. When those messengers share the language, culture, or lived experience of the families being reached, they can do more than translate words. They can build trust.
That trust matters because consent is not just a form. It is a decision parents make based on whether the program feels clear, safe, respectful, and useful. For some families, that may mean a direct conversation instead of a paper form. For others, it may mean repeated reassurance that they will not receive a surprise bill, that their child will not be forced into treatment, or that the visit will lead to real help if a problem is found.
For dental professionals and program leaders, this means using plain language, offering more than one way to respond, explaining cost clearly, respecting parents’ concerns, and helping families understand the importance of primary teeth and preventive care. It also means making sure children who need more than a screening have a real path to treatment.
School-based dental care can be a doorway into trusted, ongoing care — but only if families understand what is behind the door and believe it will truly help their child.
That is the work our members do every day. And it is why America’s ToothFairy continues to support nonprofit dental clinics and community-based providers that are not only bringing care to children, but building the relationships families need to keep coming back.
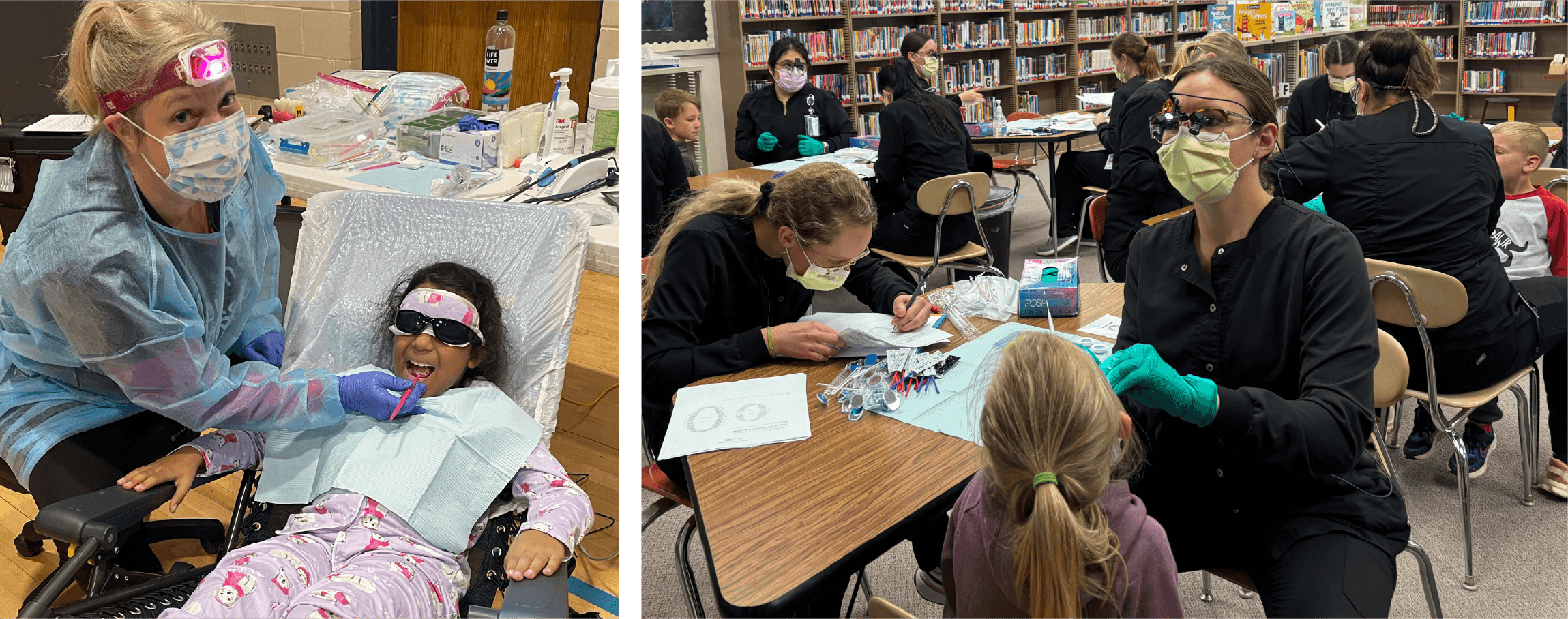
A student receives a screening at his school thanks to the staff at Let's Smile, Inc. in Owatonna, MN


